
#021: Lineage Cell Therapeutics Deep Dive
Regenerative Cell Therapies. Required Reading. Birth of an Industry.

📡 In this edition of Longevity Marketcap Telemetry
For New Subscribers
Last Week in Longevity
Longevity Futures
Lineage Cell Therapeutics Deep Dive
Tweet of the Week
*Disclaimer: None of this should be taken as financial advice. It is for educational purposes only.
🎉 A Welcome & Resources for Newbies.

Because of recent growth (thanks to Balaji Srinivasan ) many of you reading this are probably new subscribers.
Welcome, early adopters! You’re in good company.
Our subscriber base includes forward thinkers from all backgrounds: Scientists, venture capitalists, startup founders, fund managers, longevity enthusiasts, the longevity-curious, and more.
For those who might be new to longevity biotech I have collated a list of “required reading” to get you up to speed:
Short Longevity FAQ - Laura Deming: This a short ( <5 min read) overview of the main areas of research and targets to extend lifespan.
Long Longevity FAQ - José Luis Ricón: A longer more detailed FAQ that also includes a bonus primer on fundamental biology.
Juvenescence: Investing in the Age of Longevity - Jim Mellon: A book written by the patron saint of longevity investing / British billionaire. Covers both science and industry.
Lifespan: Why we age -- and why we don’t have to - David Sinclair: A book written by Professor of Genetics at Harvard and founder of Life Biosciences.
Ending Aging - Aubrey de Grey: The book that started many people down the longevity rabbit hole, myself included.
And here are some of my newsletters with general background info:
All the Longevity Therapies in Clinical Trials Today Part 1 and Part 2: We have reached an inflection point in anti-aging science. Therapies developed in the context of aging are being tested in clinical trials TODAY. Timeline Chart.
A Tour of All Senolytics Companies - The hottest area in longevity biotech -- therapies that kill harmful aged cells that have lost the ability to divide.
How to Modulate Biology- A short comparison of the main therapeutic modalities used in biotech.
FYI: Just in case you were wondering, this newsletter will be free forever (obvs). I started writing primarily so I could learn more about longevity biotechnology and educate others about it too. We need as many people as possible on board to accelerate the end of aging. Build. Invest. Educate. Share. Whatever it takes.
-Nathan Cheng @realNathanCheng
LongevityMarketcap.com // LongevityList.com // BiohackStack.com
📝 Last Week in Longevity

The launch of Nature Aging. There are several scientific journals devoted to aging but this new journal is notable. Nature is the most prestigious academic journal and their topical journals are all respected in their own right. In 1983, the first issue of Nature Biotechnology was published, right around the same time as the Genentech and Amgen IPOs. Back then it signaled the birth of an industry. And now we have a signal of a new one. Note: Amgen’s stock price has increased by 916x since 1983… 20% annualized for ~ 40 years.
Gerostate Alpha - A new anti-aging pharma startup spun out of the Buck Institute and backed by Y Combinator. Founders Simon Melov and Mark Lucanic are looking to develop new drugs outside of the “Hallmarks of Aging” box by doing high throughput screens based on many functional domains of aging combined. The company already has some promising hits (+40% C. elegans lifespan, reverse bone loss in mice) and is looking to initiate clinical trials within 2 years.
Carmat (EPA:ALCAR) gains European approval to sell artificial heart. The French company will sell their self-regulating artificial heart as a “bridge-to-transplant” temporary implant. In clinical trials, 70% of patients with the implant were able to survive past six months. One patient was able to survive 2-years with the device.
CorNeat artificial cornea restores sight to legally blind 78-year old man. The implant, made of a biomimetic material, is easier to implant and integrates better than existing cornea implants.
📅 Longevity Futures
DNA Tie Club / Biotech & Life Sciences Clubhouse Meeting 1:00 PM EST Saturday. Every Saturday Joshua Elkington (VC @ Axial) hosts a biology / biotech chat on Clubhouse. A wide range of participants from industry and academia show up regularly to discuss everything biology and biotech.
January 26- 28, 2021: 3rd Annual Longevity Therapeutics Conference. Will include speakers from Unity Biotechnology (Ned David), SENS Research Foundation (Aubrey de Grey), Insilico Medicine (Alex Zhavoronkov), Alkahest, Stealth BioTherapeutics, Lineage Cell Therapeutics (Brian Culley), Rubedo Life Sciences, Rejuversen, Laura Deming, and others. Online. Cost: $1099 - $1899.
Undoing Aging 2021 Conference May 13- 15, 2021. Berlin, Germany. Organized by Micahel Greve’s (Kizoo) Forever Healthy Foundation, this is one of the biggest longevity industry and research conferences. This year’s speakers will include Ned David (Unity Biotechnology), Steve Horvath, João Pedro de Magalhães, and others. There will also be a startup exhibition. Early bird ticket sales end March 5th.
Interested in learning more about investing in longevity biotechnology? Make sure to subscribe to receive the weekly Longevity Marketcap Newsletter. It’s free.
Lineage Cell Therapeutics Deep Dive
Reversing aging through cell replacement.
Today we are going to take a closer look at Lineage Cell Therapeutics (NYSE:LCTX). This California-based regenerative medicine company develops cell therapies derived from human embryonic stem cells. (Disclaimer: I have a small position in LCTX)
The big picture: Why are regenerative cell therapies important?
The majority of the longevity industry is focused on drugs to treat aging. These drugs interact with the molecules involved in super complex metabolic pathways, hopefully modulating biological aging in the end.
On the other hand, regenerative cell therapies can be used to replace aged and damaged components of the body. It’s the same strategy we use to maintain vintage cars and 50+ year old nuclear reactors. No need to understand the causal chain of aging or disease. We even have the technology to reprogram our adult cells into an endless supply of undifferentiated young cells (induced pluripotency). The challenge with the cellular replacement approach to treat aging is being able to manufacture the right cells at scale and get them to where they need to be (and stay there). This is much harder than it sounds.
Here is a list of some companies in the regenerative cell therapy space:
AgeX Therapeutics (NYSE:AGE): Mike West’s allogeneic progenitor stem cell + induced-tissue regeneration company.
Blue Rock Therapeutics: induced pluripotent stem cell and gene therapies.
Astellas Pharma (TYO:4503): retinal pigment epithelial cells for eye disease (similar to Lineage Cell Therapeutics).
Minovia: mitochondrial transplants for rare mtDNA mutation diseases.
Mitrix: mitochondrial transfusions to treat disease.
CRISPR Therapeutics (NASDAQ:CRSP): Developing a gene + cell therapy to cure T1 diabetes using edited pancreatic cells.
Mesoblast (NASDAQ:MESO): Mesenchymal stem cells that reduce inflammation to promote regeneration.
Athersys (NASDAQ:ATHX): Mesenchymal stem cells, again.
Longeveron: More mesenchymal stem cells.
Cellular Biomedicine Group (NASDAQ:CBMG): Guess who? Mesenchymal stem cells.
Note: There are also many companies developing traditional drugs to stimulate cell regeneration in vivo (Frequency Therapeutics, Samumed, etc).
Lineage Cell Therapeutics is one of the few publicly-traded regenerative cell therapy companies. And while the therapies they are developing are not aiming to extend maximal lifespan, they do represent a scalable localized reversal of aging and damage repair. An FDA approval here would be a monumental first step for both longevity biotech and cellular therapies. Currently there are very few FDA-approved cellular therapies.
Lineage Cell Therapeutics (NYSE:LCTX) at a Glance
Market cap: $450 M
Enterprise Value: $412 M
Founded: 1990
CEO: Brian Culley
Modality: Cell therapy, embryonic stem cell derived, allogeneic transplant.
Pipeline
Links
Most recent Webinar Presentation: H.C Wainwright Conference Jan 4, 2021
Evaluation Framework
I am using Greg Bailey’s (CEO of Juvenescence) “Five Questions” as a way to evaluate whether Lineage Cell Therapeutics is a reasonable investment. I will also include a commentary on company valuation.
Does the science make sense?
Does the company have IP protection?
Do I agree with the business plan?
Can management execute on the business plan?
Does the company have enough cash to make it to the “light switch moment”?
Does the science make sense?
Lineage Cell Therapeutics develops off-the-shelf allogeneic cells made from human embryonic stem cells (hESCs). These embryonic cells are remarkable because of their unlimited proliferative potential and their ability to differentiate into any type of cell (“pluripotency”).
By carefully exposing embryonic stem cells to specific conditions, Lineage can manufacture virtually any specific type of cell at scale. These cells can then be transplanted into patients to treat or even cure disease.
Lineage’s current therapeutic pipeline includes manufacturing and transplanting three kinds of cells:
OpRegen: Retinal pigment epithelial cells -- To treat dry age-related macular degeneration.
OPC1: Oligodendrocyte progenitor cells -- To treat spinal cord injury.
VAC2: Dendritic cells -- To treat non-small cell lung cancer via an immune therapy vaccine. Can be adapted to other cancers in theory.
Let’s take a look at the background of each pipeline separately.
OpRegen // Allogeneic Retinal pigment epithelial (RPE) cells // Dry Age-related Macular Degeneration
Saving the retina support cells to restore sight.

What is Dry Age-related Macular Degeneration?
Dry age-related Macular Degeneration (dry AMD) is a common disease that causes loss of vision in adults. Age is the primary risk factor.
The macula is the area of the retina responsible for central vision (high-resolution vision). It is roughly 5.5 mm in diameter.
Retinal pigment epithelial cells (RPE cells) form a single-cell layer behind the rod and cone photoreceptors of the retina. RPE cells are responsible for nutrient and waste transport of the photoreceptor layer, phagocytosis of spent photoreceptor outer tips, protection of the retina from high-energy light, and maintenance of retina homeostasis through signalling factors (Boulton et al. 2001)
In the early stages of dry AMD disruption of RPE cell function leads to the formation of deposits of protein and lipid cellular waste (called drusen) inside and below RPE cells. This can induce an inflammatory response. (Johnson et al. 2001). Symptoms can include visual distortion or loss of visual acuity.
Advanced stage dry AMD is characterized by the loss of retinal pigment epithelial cells leading to the thinning and loss of photoreceptors and deterioration of vision. This presents in a condition known as geographic atrophy (GA), as the growing patch of retinal cell loss resembles the shape of an island.
The exact cause of dry AMD is not known, although dysfunctional mitochondria within RPE cells as well as lipofuscin have been implicated (Fisher et al 2018)
Does this therapeutic approach make sense?
The beauty of cellular replacement therapies like Lineage’s is that the understanding of the exact cause of disease is not required to treat it. Replacing cells should be able to restore function in theory.
Age-related macular degeneration is characterized predominantly by loss of RPE cells and photoreceptors. One study suggests that in some cases photoreceptor loss precedes RPE cell loss in the progression of dry AMD (Bird et al. 2014).
My take: Transplanting functional RPE cells has a good chance of slowing the progression of retinal atrophy. Transplanted RPE cells might rejuvenate existing damaged or dysfunctional photoreceptor cells via cellular waste removal, less drusen accumulation, and homeostatic maintenance. But RPE cell transplants are unlikely to regenerate new photoreceptors. So in cases of advanced photoreceptor depletion we would not expect much therapeutic benefit. This explains why Lineage’s Phase 2 trial targets people with impaired vision, instead of those who are legally blind.
A long term cure for aging in the retina would probably require replacement of photoreceptors in addition to RPE cells. A review of different strategies for this can be found here: (Chichagova et al 2018).
What tests of RPE transplantation have been tried in the literature?
Transplantation of human embryonic stem cell-derived RPE cells into rat models of macular degeneration demonstrated rescue of degenerating photoreceptors and improved vision (Lund et al. 2006; Lu et al. 2009).
Autologous RPE + choroid cell sheets transplanted from peripheral areas of the retina to the fovea have shown improved vision in human patients. (Joussen et al. 2006)
What does Lineage’s OpRegen treatment look like?
50,000 - 200,000 RPE cells derived from human embryonic stem cells are engrafted into the back of the retina. These cells are not modified (genetically or otherwise) in any way.
A Gyroscope Orbital Subretinal Delivery System cannula is used to enter and engraft the retina from the back of the eye, obviating the need for puncturing the eye and draining the vitreous humor. The Gyroscope SDS should result in fewer adverse events associated with the surgery compared to PPV (pars planar vitrectomy) methods.
Lineage has an exclusive partnership with Gyroscope Therapeutics for this technology. Some of the earlier cohorts of the trial were given the treatment with the traditional PPV method.
Although the eye is considered immune-privileged (can tolerate foreign antigens), immunosuppressants are still given to patients around the time of the engraftment procedure (but halted within 90 days after procedure).
How strong is Lineage’s OpRegen clinical data?
Lineage is currently conducting a small Phase 1 / Phase 2a clinical trial of OpRegen -- 24 patients in total.
In the Phase 1 safety study, 12 legally blind patients were divided into 3 different dose cohorts.
Lineage reports OpRegen was well tolerated with the most common side effect being mild to moderate epiretinal membrane (ERM: scarring of the retina) due to the PPV method of engraftment.
There have not been any reports of ERM from the newer Gyroscope cannula method of engraftment.
There was one report of retinal detachment of unknown cause.
My take: Lineage has not seen any negative immune responses. The adverse events are more related to the surgical procedure itself, which can be minimized with the new Gyroscope technique.
In the ongoing Phase 2a efficacy study, 12 patients with impaired vision (20/64 - 20/250 eyesight) and dry AMD + geographic atrophy were treated with OpRegen in one eye. There are no patients in the control arm --the untreated eye serves as the control. Results:
Statistically significant increase in visual acuity (BCVA from an eye chart) relative to untreated eye at 9 months and 12 months after treatment. ~10 letters in improvement. 86% of patients saw an improvement in vision. Improvements were sustained up to 24 months in some patients. One patient saw an improvement of 25 letters (!).
Mean change in the size of geographic atrophy was trending towards slower growth compared to the untreated eye. This data is less encouraging -- geographic atrophy is still progressing. Perhaps the continued atrophy comes from the photoreceptors that are beyond repair?
One patient demonstrated a decrease in geographic atrophy area, which was sustained up to 23 months later. Lineage claims this is the first known clinical regeneration of retinal tissue.
My take: It looks like maintaining vision improvement long term might be difficult. Astellas has a very similar treatment that saw initial gains in the first 12 months before returning nearly to baseline after 36 months.
How are Lineage’s OpRegen manufactured?
Unlike small molecule drugs, cellular therapies require much more attention to manufacturing. Demonstrations of microbiological safety, cell identity, purity, potency, viability, reproducibility, and consistency are required by the FDA.
3-litre bioreactors can produce 2,500 doses of OpRegen each. Doses are administered in a cell solution of Balanced Salt Plus.
Lineage claims they can produce cell doses of 99% purity.
Manufacturing is done in-house at Lineage’s cGMP facility in Israel. Already at pre-commercial scale.
Lineage has developed a ready-to-administer / thaw-and-inject formulation that enables much simpler administration preparation and logistics. Preparation time for injection takes only 30 minutes.
OPC1: Spinal Cord Injury treatment via oligodendrocyte progenitor transplantation
Re-insulating the electrical wiring in the spine.

What is spinal cord injury? What’s the pathophysiology?
Spinal cord injury is damage to the spinal cord. It can cause loss of control and sensation in limbs and other parts of the body (bladder, sphincter, etc).
Damage can be caused by both the initial trauma and by the secondary inflammatory response to the initial trauma.
Spinal cord injury levels can be denoted using a scale according to where the injury occurred. Injuries that occur higher up on the spine are generally more disabling. (Ex. Most disabling —> C1 → C8 → T1 → T12 → L1 → L5 → S1 → S5—> least disabling.)
Spinal cord injury results in death of cells, including neurons, oligodendrocytes, astrocytes, and precursor cells. Demyelinated axons have been observed up to a decade after injury. (Thuret et al. 2006)
Does this therapeutic approach make sense?
Lineage is transplanting oligodendrocyte progenitor cells into the spine to regenerate tissue and restore motor function. They hope to allow patients to regain control of their upper limbs and require less assistance with daily life.
Oligodendrocytes are central nervous system cells that are responsible for generating the myelin that serves as electrical insulation and support for the axons (the long spindles) of neurons. It is also believed loss of oligodendrocytes may cause axon degeneration independent of demyelination (Oluich et al. 2012).
A progenitor cell is a type of stem cell that can differentiate into only a few different types of cells and cannot replicate indefinitely.
Oligodendrocyte progenitors can differentiate into oligodendrocyte cells or astrocytes. Astrocytes are central nervous system cells that have many different support functions including maintaining homeostasis and tissue repair.
Based on preclinical studies, Lineage believes OPC1 works to restore motor function by myelinating axons, remodelling tissue, prevention of lesion cavities, and secretion of factors that support neuron survival.
Lineage’s approach seems reasonable, though, given the complexity of the central nervous system, it is not clear that oligodendrocyte progenitors alone will be sufficient to repair all the damage in human SCI patients. Perhaps regeneration of cells other than oligodendrocytes and astrocytes will be required.
From a safety standpoint, the biggest risk for this therapy is that the transplanted oligodendrocytes could migrate into the brain. Engraftment stability is crucial.
How strong is Lineage’s OPC1 clinical data?
In Lineage’s open-label Phase 1/2a “SCiStar” study, 25 patients with spinal cord injury were tested with three sequential escalating doses of up to 20 million OPC1 cells, 21- 42 days post-injury. Results:
No severe adverse changes detected in MRI scans, even after 2 year follow up.
96% successful and stable engraftment, no degradation in condition. Tissue matrix was formed at injury site and no cavitation lesions were observed.
32% of patients improved 2 motor levels or more
64% of patients improved 1 motor level.
One patient achieved an improvement of 3 motor levels.
Patient story: Lucas Linder was paralyzed from the neck down after a car crash. After OPC1 treatment he regained the ability to type, throw a baseball, hand movement, etc.
What does Lineage’s OPC1 treatment look like?
20 million oligodendrocyte progenitor cells derived from human embryonic stem cells (H7 line) injected into the spine. Three sequentially escalating doses placed in Balanced Salt Solution.
Low-level immunosuppressant drug taken for 60 days after procedure.
OPC1 Manufacturing Update
New ready-to-inject formulation.
Increased production scale 10 - 20x
Eliminated all animal-based products and reagents.
Reduced impurities.
Production moved to cGMP facility in Israel.
Developing new delivery procedure / device
VAC2: Non-small cell lung cancer treatment with dendritic cells
A potential cancer treatment platform. Developed in partnership with Cancer Research UK.
What is non-small cell lung cancer (NSCLC)?
The more common form of lung cancer. Usually caused by smoking. 5-year survival rates for NSCLC cancer is 24%.
Lineage’s VAC2 platform can be adapted to other cancers as well.
Does this therapeutic approach make sense?
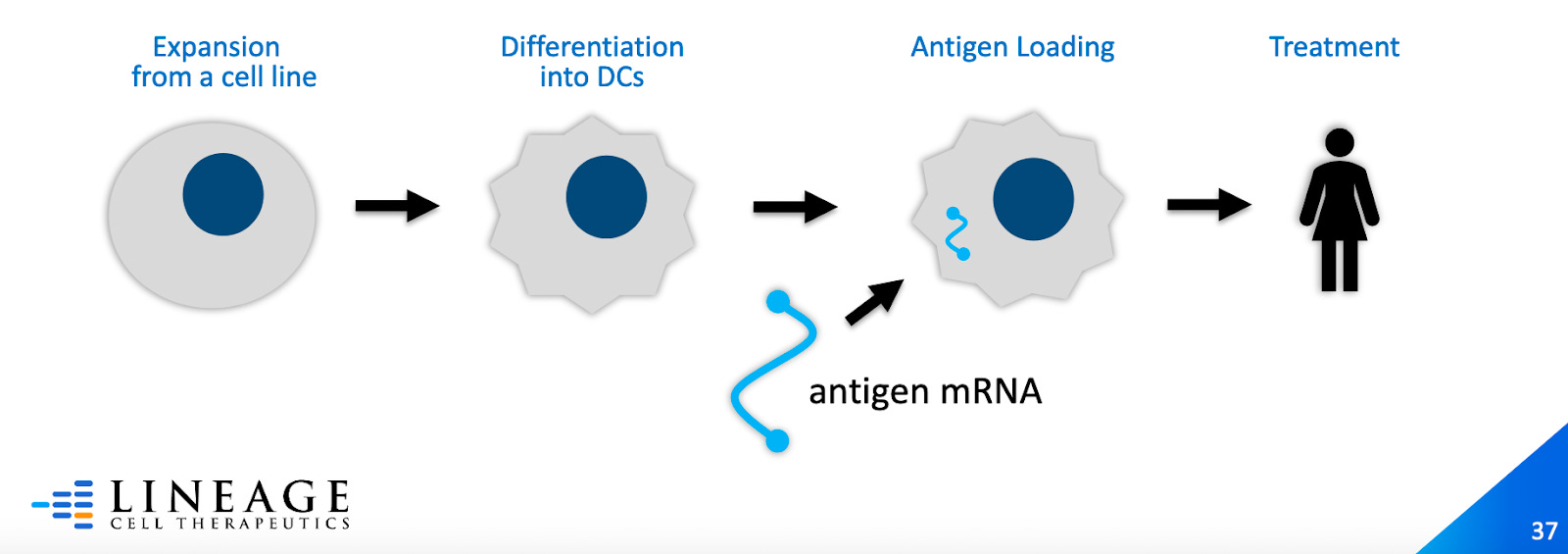
Lineage is developing a cancer vaccine by loading dendritic cells with tumour antigens. The cells are injected into the body, which trains the patient’s immune system to attack tumours that have this antigen.
Dendritic cells are immune cells that serve as the bridge between the innate and adaptive immune systems. They capture, process, and present antigens on their surface to activate T cells.
VAC2 uses allogeneic dendritic cells loaded with the hTERT (human telomerase reverse transcriptase) tumour antigen. hTERT is a component of telomerase -- a protein that cancer cells use to lengthen their telomeres in order to divide without limit.
Dendritic cell cancer vaccines are not new. Provenge, the first dendritic cell cancer vaccine, was approved by the FDA in 2010 -- the first and only cellular cancer vaccine to this day. It modestly increases survival of prostate cancer patients
The main challenges for dendritic cell cancer vaccines include insufficient antigen presentation and inability to withstand the immunosuppressive tumour microenvironment. Strategies combining dendritic cancer vaccines with other therapies (checkpoint inhibitors, etc) are being tested.
Dendritic cell therapies are generally expected to be safe.
Lineage’s VAC2 clinical data.
A Phase 1 trial is currently ongoing to test the safety and (beneficial) immunogenic response in NSCLC patients.
Early data suggest that the safety profile so far is excellent and the vaccine elicits a high level of antigen-expressing T cells.
What does Lineage’s VAC2 therapy look like?
Up to six vaccinations over six weeks. Each vaccination contains 10 million dendritic cells loaded with the hTERT antigen.
An HLA (human leukocyte antigen) pre-screening test will be used. The vaccine only works with patients that express a certain HLA.
Does the company have IP protection?
I’m not a patent lawyer so this section will be difficult for me to appraise.
Lineage has a large number of patents, particularly in the human embryonic stem cell space. Most of these patents are held through their subsidiaries.
Lineage’s OpRegen program has patents owned through their subsidiary CellCure Neurosciences that expire from 2025 - 2033. Lineage successfully defended two of their European OpRegen patents in 2017. See patents here.
Lineage’s OPC1 program has patents regarding the differentiation of human embryonic stem cells into neural cells, purification and culture methods. These patents expire from 2021 - 2038.
Do I agree with the business plan?
Let’s examine the business case for each pipeline.
OpRegen // Dry age-related macular degeneration.
Age-related macular degeneration (Wet + Dry forms) affects ~ 11 million people in the United States alone.
Wet AMD accounts for only ~10% of total AMD cases. Dry AMD is ~ 90% of cases. The market for (wet) AMD treatments is forecasted to grow at a CAGR of 8.1% according to GlobalData. Addressable market is growing due to aging demographics.
Dry AMD (which Lineage is targeting) has a high unmet need. There are no FDA approved therapies for dry AMD. Lineage believes the market for Dry AMD treatment could be ~ $10s of billions a year.
Competitors:
Astellas is developing a very similar hESC-derived RPE cell replacement therapy as well. Like Lineage, their treatment saw improvements in visual acuity, but after 36 months Astella’s patients were nearly back to baseline.
An RPE cell patch implantation therapy developed by Amir Kashani at USC has also seen similar levels of vision improvement as Lineage’s treatment. See here for more cellular treatments being tested for AMD.
Many drugs are also being developed to treat dry AMD including, neuroprotectors, mitochondrial targeting drugs (Stealth BioTherapeutics, another longevity company), and visual cycle modulators.
OPC1 // spinal cord injury
Affects 18,000 people a year in the U.S.
There are no FDA approved treatments for spinal cord injury. High unmet need.
Lifetime care can cost up to $5 million per patient
Global spinal cord injury market may grow to $3 billion / year by 2025.
Approved for Orphan Drug Status (7-year tax-free window + exclusive right to develop a cure).
VAC2 // cancer vaccine
The number of therapies for treating non-small cell lung cancer is manifold. Lung cancer is the 2nd most common form of cancer.
The global market for non-small cell lung cancer is projected to rise to $43 billion in 2026.
VAC2 may end up being used in combination with other leading cancer drugs (immunotherapies, chemotherapies, etc).
Lineage recently stated they are open for partnerships. Given their cash situation this a prudent strategy. It seems like they want to avoid a stock offering. I would like to see them continue to develop new cellular replacement therapies for other age-related diseases.
Valuation
Andy Jones published an analysis of Lineage Cell Therapeutics in July 2020 (also check out the comments section of his article for an interesting discussion). The report included a Present Value calculation and Discounted Cash Flow (DCF) analysis of the company based on some future revenue projections. Here are the assumptions and final results in Jone’s calculation:
Net Present Value (NPV) Estimate:
Cash flow positive by 2023 based on analyst estimates of future revenue.
High 30% discount rate for early-stage biotech.
Conservative Industry Average Price / Sales of 5
Present Value = $2.39 / share
Discounted Cash Flow Estimate
Selling, General and Administrative expenses = 34% of Revenue
Marketing expenses = 5%
Cost of Goods Sold (COGS) = 10%
Odds of approval = 18%
OpRegen
Market share = 40%
Market size = ~$4B
OPC1
Market share = 40%
Market size = $6B
VAC2
Peak sales = $1.7B
Fair Value = $1.69 / share
At the time of Jone’s analysis, Lineage Cell Therapeutics was trading at ~$0.94 per share. He concluded that based on even his very conservative valuation estimates that Lineage was severely undervalued. As of this writing, Lineage is trading at $3.00 / share.
Do I believe management can execute on the business plan?
A Brief History of BioTime. Brian Culley, take the wheel.
Lineage Cell Therapeutics (formerly BioTime) was founded in 1990. In the early 2000s, the company commercialized a low-temperature blood volume expander (Hextend) with intent for future application in cryonics.
Around 2006, the company pivoted to regenerative medicine with a focus on stem cell therapies. Mike West, a pioneer in stem cell research, was CEO during this time.
In 2018, Mike West left BioTime to become the CEO of AgeX Therapeutics (at that point a subsidiary of BioTime, Lineage has since divested)
Currently, the company is helmed by Brain Culley who joined as CEO in 2018. Under Culley’s leadership, the company has leaned out by selling off stakes in their subsidiaries (AgeX and OncoCyte), narrowed their focus on advancing their clinical programs, and rebranded to Lineage Cell Therapeutics.
Culley’s strategy appears to rely on low cash burn and reliance on funding from government / non-profit organizations for clinical trials.
Culley has 25+ of experience in life science industry and academia. He was formerly the CEO of two publicly listed biotechnology companies: Mast Therapeutics and Artemis Therapeutics. Check out Culley’s interview on The Simple Biotech Podcast.
My take: Culley seems competent enough to get them to what I presume will be an eventual buyout or partnership if their programs are successful. Currently, they do not have any other early-stage programs to develop further -- though their VAC2 dendritic cell cancer vaccine could be expanded to other cancer indications.
Does the company have enough cash to reach the “light switch” moment?
Sort of.
According to Lineage’s most recent 10-Q filing, they have roughly $33 million in cash and $5 million in marketable securities. This should allow the company to continue operations until 2022 to get the readouts for their current clinical trials.
Lineage’s current clinical trials were small (Phase 2a) and larger trials will be needed. This will require much more cash.
Lineage has received many grants to fund its research. The California Institute for Regenerative Medicine provided Lineage with $14M for OPC1 and it sounds like the company expects continued funding. Lineage has received similar-sized grants from the Israeli Innovation Authority and Cancer Research UK. The company is also considering seeking funding from the Christopher Reeves Foundation to fund their OPC1 spinal cord injury trial.
Lineage may end up partnering with a bigger company before they require more cash. Culley has mentioned they are open to such partnerships.
Future Outlook for Lineage Cell Therapeutics

Lineage has a several clinical data updates in Q2 and Q3 of this year concerning their OpRegen and VAC2 trials. They are also planning to meet with the FDA this year to discuss the design of their next clinical trial for OPC1.
Overall, I like the company. Regenerative cell therapies hold incredible potential for treating disease. As manufacturing and transplantation techniques improve there may be opportunities to make more significant progress to treat aging with these therapies.
I have a small speculative position in Lineage -- only as much as I am willing to completely lose. I intend on holding it as long as the company is still developing biotechnology relevant to longevity.
Tweet of the Week
Laura Deming was asked this question during a Clubhouse session this week (and many other times I presume). She doesn’t recommend anything. Neither does Aubrey de Grey (other than donating to SENS!).
However, there are many researchers, investors, and founders in longevity that do dabble in personal longevity “stacks”. David Sinclair (Professor at Harvard, founder of Life Biosciences) and Robert Nelson (VC at ARCH Venture Partners) take metformin and NMN, among other things. Jim Mellon has written that he takes Elysium’s Basis.
It’s quite a conundrum.
Hopefully in the next five years we will get much more clarity on the efficacy of metformin, NAD+ boosters like NMN and NR, alpha-ketoglutarate, rapamycin, etc. And if we are lucky, some new anti-aging compounds too.
Hey Nathan,
Have you ever looked into Eidos Therapeutics? Seems to me like a good candidate to be added to your list of longevity stocks.
Cheers